
The Fundamentals of Erection 101
An erection, colloquially referred to in a variety of terms, is actually a complex physiological process that entails much more than what these simple monikers suggest. It could be likened to the intricate engineering of a rocket. Achieving an erection isn’t akin to the science of space exploration, but it does require the harmonious functioning of multiple complex systems, similar to the elements found in rocketry—robust materials, precise mechanics, and intricate controls—all within the penile structure.
How the Penis Grows in Size
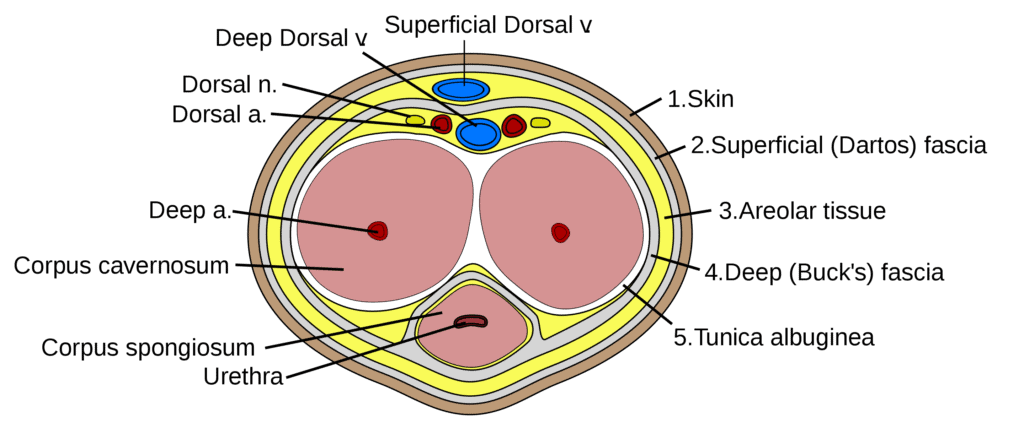
The Structural Composition The penis consists of three cylindrical tissues. Two of these cylinders, known as the corpora cavernosa, are aligned side by side and form the main bulk of the penis when erect, filling with blood to enable this state. The third, situated beneath the first two, encompasses the urethra—the conduit for urine—and extends to form the glans penis, also referred to as the head of the penis.
These shaft cylinders, the corpora cavernosa, are encased in the tunica albuginea, a term derived from Latin describing one of the body’s most resilient and flexible tissues. The tunica albuginea, similar to a tunic in ancient Roman attire, provides a robust yet elastic sheath for the erectile tissue.

The tunica albuginea, a remarkable tissue surrounding the penile cylinders, enables the penis to swell and stiffen substantially during arousal. This is due to the cylinders filling with blood—multiplying in volume up to two to five times their flaccid size—rather than air, which allows the penis to expand significantly while achieving the firmness of an inflated tire. Individuals vary in their penile expansion capacity, colloquially termed as “showers” and “growers.”
Showers have a less pronounced change between flaccid and erect states, often appearing larger at rest, while growers experience a notable increase in size during erection.
The veins responsible for the outflow of blood are strategically situated within the walls of these cylinders. As the cylinders engorge and the internal pressure mounts, these veins are compressed, effectively sealing the blood within to maintain an erection. This internal pressure surpasses the general blood pressure in the circulatory system, preventing further influx of blood.
Adding to the mechanism, at the base of the penile cylinders are the ischiocavernosus muscles, which, upon contraction, exert additional pressure on these regions. This action serves to intensify the rigidity and fullness of the erection, resulting in the heightened sensation often described as a pulsating or throbbing state.

Exploring the Inner Workings of the Penis
The resilience of the penile shaft owes to the tunica albuginea, a sheath that envelops the penile cylinders with a distinctive configuration unmatched elsewhere in the body. This sheath is composed of collagen fibers, a robust tissue also found in our skin, blood vessels, and tendons, which provides them with strength and elasticity.
However, in the tunica albuginea, these fibers are uniquely organized: woven into spiraling bands that encircle the cylinders, coupled with additional layers of longitudinally oriented fibers extending along the shaft. Interspersed with approximately 5% elastic fibers, similar to the material in the waistband of undergarments, this intricate meshwork allows for the penis to stretch and expand, yet become impressively firm and resistant to bending or buckling forces during sexual intercourse.
Tunica spongiosum, the third cylinder encompassing the urethra and culminating in the glans, lacks this complex multi-layered structure. It permits stretching but not the same degree of hardness as the penile shaft, which is beneficial as it allows for urination even during an erection by preventing the urethral passage from being occluded by excessive pressure.
This design mitigates the difficulty of urination when aroused—a common inconvenience—but does not entirely prevent it, a phenomenon distinct from the temporary urinary hesitance often experienced post-coitus.
Summary
- During arousal, the tunica albuginea enables the penile cylinders to swell with blood up to five times their flaccid size, leading to an erection; this varies among individuals, with “showers” having less dramatic changes and “growers” significantly enlarging. The blood is trapped inside by the compression of outflow veins by the engorged cylinders, surpassing the body’s blood pressure.
- The ischiocavernosus muscles at the base of the penile cylinders contract to further increase the rigidity and fullness of the erection, enhancing the sensation to a pulsating or throbbing state.
- The tunica albuginea’s unique arrangement of collagen and elastic fibers allows the penis to expand and become firm during sexual activity, while the tunica spongiosum around the urethra permits stretching without as much hardness, allowing for urination even with an erection and preventing the urethral passage from being closed off.

Blood Circulation of penis
The vascular network within the penile structure functions akin to hydraulic lines, vital for facilitating blood flow. The penile arteries are extensions of the larger arterial system that services the pelvis and lower limbs. These arteries trace a path beneath the ischial tuberosities — the sitting bones — and progress toward the root of the penile cylinders, which are firmly attached to the inferior aspect of the pubic bone.
An intriguing anatomical detail is that the penile shaft extends internally to the same extent as it is externally visible, suggesting that the actual length of the penis is double what is externally apparent. The arteries that supply the penis are relatively narrow, with a diameter of approximately 1 millimeter, quite small in comparison to the coronary arteries that fuel the heart and are about five times larger in diameter.
This size discrepancy illustrates why erectile function is often one of the first faculties to decline with vascular aging, potentially serving as an early indicator of cardiovascular disease. Nevertheless, in a state of good health, these slender arteries are perfectly adequate for penile blood supply.
Each penile artery bifurcates into three primary branches that deliver blood to the erectile cylinders and the spongiosum that encompasses the urethra and forms the glans. One of these branches ascends along the dorsal aspect of the shaft, supplying the penile skin, subcutaneous tissue, and the glans.
Due to the very small penile arteries why erectile function is often one of the first faculties to decline with vascular aging, potentially serving as an early indicator of cardiovascular disease.

Regulation of Blood Flow
Under typical conditions, there is a consistent, albeit reduced, flow of blood to the penis. During an erection, this flow is significantly enhanced. Arterial flow modulation is achieved through the contractile activity of the muscular layer within the artery walls, akin to the mechanism of a faucet controlling water flow — constricting to diminish flow and relaxing to increase it.
The autonomic nervous system, specifically the sympathetic nerves, governs the dilation and constriction of these arterial muscles. These nerves, which function autonomously from conscious control, are analogous to traffic controllers, meticulously managing blood distribution throughout the body. Embedded along the arterial walls, sympathetic nerves secrete adrenaline and noradrenaline, which influence the arterial muscles to either dilate or contract, thus regulating blood flow according to the physiological demands of different body regions.
Adrenaline and its Effects on the penis
Adrenaline, a potent hormone, is secreted not only by nerve endings but also by the adrenal glands, which are small, lipid-rich structures perched atop the kidneys. Its primary role is to prime the body for ‘fight or flight’ responses in the face of perceived threats.
This hormone orchestrates a series of physiological adjustments, including the dilation of blood vessels that serve essential organs such as the muscles, liver, heart, and brain, prioritizing their function during critical situations. Conversely, it constricts the blood vessels leading to less critical areas, such as the extremities and, notably, the penis.
The impact of adrenaline includes an accelerated heart rate and expanded lung capacity, which are beneficial for immediate survival. However, these effects come at the expense of penile erection, which is inhibited during adrenaline surges. Such a rush can be triggered by actual or perceived threats, psychological stress, or anxiety, irrespective of the stimulus, the result on penile function is the same.
A primal example is our ancestors’ response to predatory threats, where an adrenaline surge would understandably redirect bodily functions away from sexual arousal. Similarly, contemporary stressors or performance anxieties can provoke the same physiological reaction.
In the absence of stress, danger, or anxiety, the body’s sympathetic nervous system — the ‘traffic cop’ of nerves — reduces its regulatory actions, allowing blood vessels to relax and blood flow to resume unimpeded to all parts of the body, including those previously restricted areas like the fingers, toes, and penis.
Summary in short
- The penile vascular network is crucial for blood flow, with arteries stemming from the pelvis, running under the sitting bones, and extending into the penile tissue which is as long internally as it is externally, yet these arteries are narrow at about 1 millimeter in diameter, making them sensitive indicators of vascular health.
- These penile arteries branch into three main arteries that supply blood to the erectile tissue and the spongiosum, with one branch specifically delivering blood to the dorsal side, affecting the penile skin and glans.
- Blood flow to the penis is typically low but increases substantially during an erection through a process regulated by the autonomic nervous system, which adjusts arterial muscles like a faucet to control the flow based on the body’s needs.
- Adrenaline, produced by nerve endings and adrenal glands, triggers the ‘fight or flight’ response, dilating blood vessels for key organs but constricting them for the penis, impacting erections especially during stress, while the sympathetic nervous system otherwise ensures balanced blood distribution to all body parts, including the extremities and penis, in non-stressful conditions.
Vascular Mechanics of Erectile Function
The functional anatomy of penile erection is reliant on the penile artery’s middle branch, a vital vessel that penetrates the shaft of the penis. The shaft’s interior resembles a finely textured sponge, due to the intricate network of tiny vessels and cavities that fill with blood. These cavernous structures, which could be likened to the intricate workings of a precision-engineered hydraulic device, are the driving force behind the erectile process.
The innermost cavities are coated with two distinct layers, integral to their function. The inner lining, known as the endothelium, comprises cells specifically designed to prevent blood clotting, even when blood flow is minimized during an erection. This feature is crucial; without it, stagnant blood within an erection could coagulate, leading to potentially serious complications.
Conversely, the outer layer, constituted of smooth muscle, is exceptionally responsive. This muscle layer has the remarkable ability to relax and expand, allowing the cavernous spaces within the penis to engorge with blood, thereby increasing intracavernosal pressure.
This process effectively compresses the venous outflow, securing blood within the penis to maintain an erection. In its alternative state, the muscle layer can constrict, expelling blood to dissipate the erection or maintaining a contracted state to prevent an erection from occurring.
Neurological Regulation of Erectile Response
The regulation of erectile function involves a complex interplay between two types of autonomic nerves: the parasympathetic and sympathetic nervous systems, which operate beyond voluntary control. Parasympathetic nerves facilitate the relaxation of penile smooth muscles, prompting the cavernous spaces to dilate and engorge with blood, thus inducing an erection. These nerves navigate through the pelvic region, passing between the prostate and rectum, and eventually integrate with the base of the penile shaft. Conversely, the sympathetic nerves have the opposite effect, inducing smooth muscle contraction to reduce blood flow to the penis. This dynamic constitutes a perpetual physiological tug-of-war that determines the state of penile tumescence.
Nitric Oxide: A Crucial Vasodilator
The role of nitric oxide (NO) in vascular biology is akin to its function in industrial and automotive contexts, where it facilitates explosive reactions and high-speed racing, respectively. Similarly, in the human body, NO is an essential vasodilator pivotal for blood circulation.
The primary function is to cause the smooth muscles within the penile arterial walls and erectile tissue to relax, enhancing blood flow to engender an erection. Parasympathetic nerve endings release NO directly onto the smooth muscle cells, and endothelial cells lining the erectile tissue also contribute to the NO supply.
The transient presence of NO in the smooth muscle activates a biochemical cascade that limits calcium entry into the cells and sequesters intracellular calcium within the endoplasmic reticulum.
This reduction in intracellular calcium allows the smooth muscle fibers to relax, thereby expanding the erectile spaces and permitting the influx of blood required for an erection.
Furthermore, NO is integral to the mechanism of action for erectile dysfunction medications such as Viagra, Cialis, Levitra, and Stendra. These pharmaceuticals enhance the duration and effect of the body’s natural NO, thus prolonging smooth muscle relaxation and increasing penile blood flow. They achieve this by inhibiting the enzyme phosphodiesterase (PDE), which typically deactivates NO’s effects. If not for the modulating action of PDE, a persistent erection could ensue. Therefore, these medications effectively extend the vasodilatory impact of NO, sustaining erectile function.
Summary in short
Vascular Mechanics of Erectile Function:
- The penile artery’s middle branch is crucial for penile erection.
- Inside the penis, a network of tiny blood vessels and cavities resembling a sponge fill with blood to create an erection.
- The cavities are lined with two layers: the endothelium (inner layer) and a layer of smooth muscle (outer layer).
- The endothelium prevents blood clotting, ensuring blood within an erection does not coagulate.
- The smooth muscle layer can relax and expand to allow blood to engorge the penis, or constrict to dissipate an erection.
Neurological Regulation of Erectile Response:
- Autonomic nerves control erectile function without voluntary input, comprising parasympathetic and sympathetic nervous systems.
- Parasympathetic nerves cause penile smooth muscle relaxation, allowing the penis to fill with blood and become erect.
- These nerves pass through the pelvis between the prostate and rectum, reaching the penile shaft’s base.
- Sympathetic nerves induce the contraction of smooth muscles, decreasing blood flow to the penis.
Nitric Oxide’s Role:
- Nitric oxide (NO) is essential for vascular biology, functioning as a vasodilator necessary for blood circulation and erections.
- It triggers the relaxation of penile smooth muscle and arterial walls, thus facilitating blood flow for an erection.
- NO is released by parasympathetic nerve endings and endothelial cells into smooth muscle cells.
- NO’s presence initiates a process that reduces calcium in the cells, allowing smooth muscle fibers to relax and the erectile tissue to expand with blood.
Impact of NO on Erectile Dysfunction Medications:
- Medications like Viagra, Cialis, Levitra, and Stendra extend the effect of NO.
- They inhibit the enzyme phosphodiesterase (PDE), which would otherwise limit NO’s effects, potentially causing persistent erections.
- By blocking PDE, these drugs prolong the vasodilatory impact of NO, aiding in the maintenance of an erection.

Autonomous Erectile Control
Understanding the physiological mechanisms of erectile function reveals a sophisticated system resembling a dual command structure: local reflexive responses and higher-level cerebral oversight. The analogy of a rocket with both onboard controls and a distant mission control is pertinent in describing the interplay between local reflexes and brain-mediated responses in penile tumescence.
Local penile reflexes can induce erections independent of conscious thought, responding to tactile stimulation through a neural pathway that connects the sensory nerve endings of the penis with the sacral spine. These signals may bypass the brain entirely, leading to spontaneous erections, which can occur in various everyday situations or even in individuals with spinal cord injuries, illustrating the reflexive nature of this system.
The brain, akin to a mission control center, integrates sensory inputs from all over the body and processes them through various conscious and unconscious layers. The processing centers regulate autonomic responses, which can either facilitate or inhibit an erection by modulating parasympathetic and sympathetic nerve activity. Signals from the central nervous system can instigate the erection process by stimulating the release of nitric oxide in the penile tissue or halt it by inducing vasoconstriction through adrenaline release.
Multisensory Stimulation
The induction of an erection typically involves the stimulation of multiple senses, with sight often playing a critical role. Visual stimuli are processed in the occipital lobe and disseminated throughout the brain, interacting with memory, emotional centers, and areas outside conscious control. The release of neurotransmitters such as dopamine and oxytocin from these regions then influences the initiation of an erection.
Conversely, negative sensory experiences can activate brain regions that preempt an erection by triggering a sympathetic response, culminating in an adrenaline surge that counteracts the erectile process.
The brain can independently generate the impulses for an erection through fantasy, memory, or thought, demonstrating its autonomy from direct sensory input. The hormonal milieu, particularly testosterone, plays a supportive role in maintaining sexual desire and tissue health.
Serotonin and Sexual Function
While various mechanisms serve to facilitate an erection, the brain frequently exercises restraint through serotonin release, which has an inhibitory effect on erectile function. This neurochemical not only moderates mood but also impacts sexual appetite, explaining the sexual side effects commonly associated with certain antidepressants.
Seretonin Kill erection
Higher brain functions, particularly those located in the frontal and temporal lobes, are constantly at work to modulate sexual behavior and erection through a complex array of inhibitory signals. This overarching control explains phenomena such as nocturnal erections, which occur during sleep when these regulatory centers are less active.
In certain pathological conditions where these brain regions are compromised, individuals may experience disinhibition of sexual behavior, highlighting the role of the brain in tempering sexual activity to align with socially and personally appropriate contexts.
Comprehension of the erectile process demystifies it, reducing anxiety and enabling more effective problem-solving when issues arise. Recognizing the interplay of physical, chemical, and psychological factors underscores the importance of maintaining overall health to preserve erectile function and sexual well-being.
Summary in short
- Erectile function operates through a dual system involving local reflexes that can trigger erections without conscious thought via a neural pathway from the penis to the sacral spine, and higher brain functions that can facilitate or inhibit erections through neurotransmitters and hormones like nitric oxide or adrenaline.
- Multisensory stimulation, including visual stimuli, affects the erectile process; the brain can independently generate erection impulses through fantasy or memory, influenced by neurotransmitters like dopamine and oxytocin, while testosterone maintains sexual desire and tissue health.
- Serotonin acts as a moderating neurotransmitter that can inhibit erectile function, which explains why antidepressants can have sexual side effects; the frontal and temporal lobes of the brain exert regulatory control over sexual behavior, which is less active during sleep, leading to nocturnal erections, and in cases of brain impairment, sexual inhibition can be compromised.


